- Call Us:- +91 7326070444 / +91 674 2913291
- Mon - Fri: 09.00AM to 06.00PM
Our Services

- Hydrogeological Investigations
- Hydrogeochemical Investigations
- Geophysical Investigations
- Groundwater Modelling
- Remote Sensing and GIS
- Managed Aquifer Recharge (MAR)
- Geochemical Indexing
- Human Health Risk Assessment
- Hydrological Investigations
- Sediment Transport Modelling
- Human and Climate Impact Studies
- Environmental Impact Assessment (EIA)
- Policy Design and Analysis
- Research Consultancy
- Need-based Training
Heavy Metals and Their Source Apportionment in a Tribal Stretch infected with Chronic Kidney Disease of Unknown Etiology (CKDu): An Appraisal
Chronic Kidney Disease of Unknown Etiology (CKDu) is an emerging global health challenge that continues to spread rapidly. While precise global infection statistics are unavailable, CKDu is considered an offshoot of Chronic Kidney Disease (CKD), which currently affects approximately 850 million people worldwide (Nature, 2024). It contributes to an annual mortality rate of 2.6 million, including 1.2 million deaths directly due to CKD and 1.4 million resulting from cardiovascular complications induced by impaired kidney function (GBD Chronic Kidney Disease Collaboration, 2020). CKD is now recognized as the third most rapidly increasing cause of global disease burden, and it is projected to become the fifth leading cause of death by 2040 (Foreman et al., 2020). These alarming trends have elevated CKDu as a subject of significant global interest.
A particularly troubling aspect of CKDu is its disproportionate impact on poor agricultural workers, who toil for long hours under intense heat in low-income regions. Even the global authority Kidney Disease: Improving Global Outcomes (KDIGO) has not yet reached a consensus on the disease’s underlying cause or standardized diagnostic criteria. As a result, affected patients are often left dependent on the prognostic capabilities of healthcare providers, with diagnoses frequently delayed until the disease becomes irreversible. In this context, any research that aims to uncover the etiology of CKDu makes a novel and valuable contribution to global health science.
Numerous environmental and lifestyle-related factors have been proposed as potential contributors to CKDu, including groundwater contamination, heavy metals, pesticide and herbicide exposure (including glyphosate), burnt cane harvest, alcohol consumption, contaminated diets, trace-metal deficiencies, mycotoxins, tobacco use, physical labor, heat stress, dehydration, herbal remedies, excessive use of NSAIDs, hypertension, infections, diabetes, and genetic susceptibility. These factors tend to be region-specific, each influenced by local environmental and socio-economic conditions.
In the Indian context, particular attention has been paid to the presence of fluoride, silicon, phenols, phthalates, and heavy metals such as mercury, strontium, cadmium, and lead in drinking water. Heavy metals have also been investigated in connection with CKDu in Sri Lanka, Latin America, the Balkan Peninsula, and Nigeria, as well as in Indian states like Goa, Karnataka, Odisha, and Andhra Pradesh. This has led to the formation of two opposing schools of thought: one supporting a dominant role of heavy metals in CKDu’s etiology, and the other challenging that hypothesis.
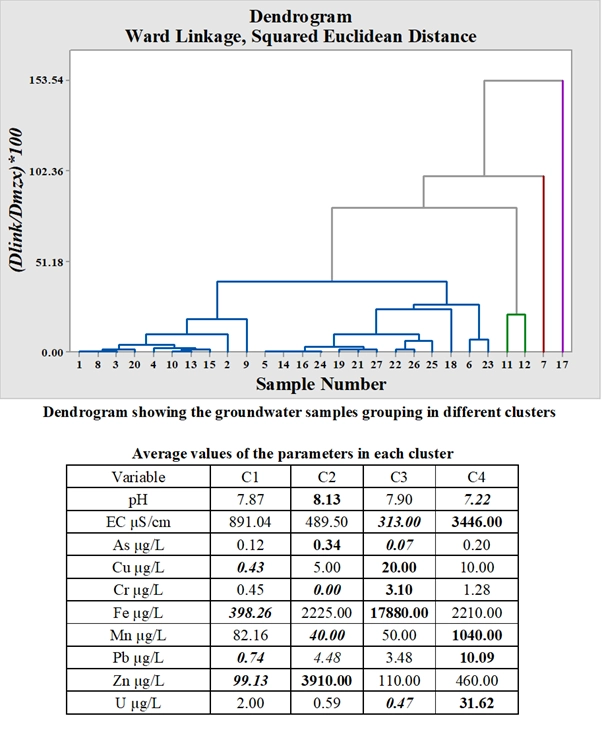
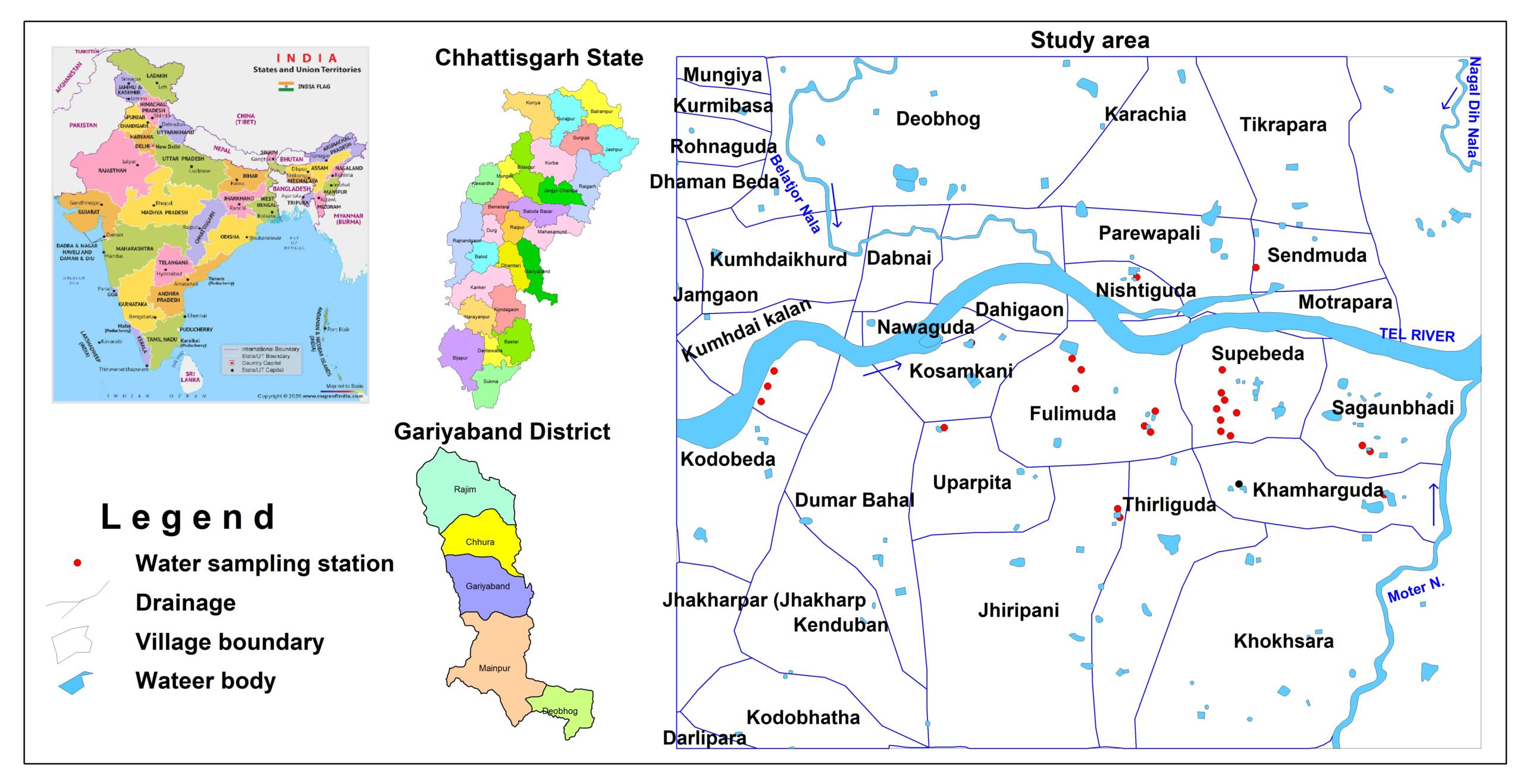
The present study seeks to test these competing hypotheses in Supebeda, a tribal village in Chhattisgarh, central India—where four prior studies by our team on CKDu have already been completed. The focus is on eight commonly occurring heavy metals in groundwater: arsenic (As), copper (Cu), chromium (Cr), iron (Fe), manganese (Mn), lead (Pb), zinc (Zn), and uranium (U).
A range of analytical techniques is being employed in this investigation:
- Heavy Metal Contamination Index (HCI) to assess groundwater quality;
- Non-carcinogenic, carcinogenic, and radiological risk assessments across multiple exposure pathways (ingestion, and dermal absorption);
- Health risk assessments for stratified population groups (infants, children, teenagers, and adults), using both deterministic and probabilistic models;
- Age-dependent ingestion dose calculations; and
- Chemometric analyses for source apportionment of heavy metals in groundwater.
The final results of this comprehensive evaluation are currently awaited.